



Study design and participants
We used a part of the prospective cohort data obtained from the Korean Social Life, Health and Aging Project (KSHAP), which was collected across three waves: wave 1 (2011), wave 4 (2015–2016), and wave 5 (2018–2019)31,32. Response rates for the main interview were 94.7%, 96.5%, and 89.6% for Waves 1, 4, and 5, respectively. For the physical health examinations—which provided the biomarker data used in this study—the response rates were 85.7%, 77.8%, and 74.5%, respectively. Older adults (aged 60 years or older in 2011) and their spouses were eligible to participate in the face-to-face survey and clinical assessment.
Sociocentric (global) network data from an entire village were collected during the survey, and biomarkers were collected during the clinical examinations31. Sociocentric network data aim to capture the social ties of everybody in a given target population, not just the sample of the population of interest. Given that the lowest response rate was 89.6%, we are confident our data adequately captures the global social networks of the entire village. This sociocentric data enables us to examine the educational level of the social ties across varying social distances: in other words, we can probe the role of the educational level of friends, friends of friends, friends of friends of friends, and beyond.
Township K is a typical rural Korean village where farming is the primary industry. With the aid of the public officers of township K and a pilot study, 860 individuals aged 60 or older and their spouses were identified as the KSHAP population. The face-to-face survey was completed with 814 out of the 860 target residents during wave 1, with a response rate of 94.7%. The final analytic sample consists of 709 individuals after excluding those with missing covariates, respondents younger than 60 years old, those with diagnosed cardiovascular diseases, and those whose social network size equaled zero. Respondents were educated on the nature of the survey and written informed consent was obtained from all participants and/or their legal guardian(s) before survey completion. The institutional review board of Yonsei University approved this study, and all research was performed in accordance with relevant guidelines and regulations (YUIRB-2011-012-01 in 2011; 7001988-201806-HRBR-244-04 in 2015; 7001988-201812-HR-505-02 in 2018).
Measures
Cardiac biomarkers
We used Troponin I, BNP, and NT-proBNP biomarkers collected during health assessments in 2011, 2015–2016, and 2018–2019. Blood samples were collected from the antecubital vein after an 8-hour fasting period. They were immediately stored in a -20 °C fridge until further analysis. The concentrations of Troponin I, BNP, and NT-proBNP were quantified using the Human Cardiovascular Disease (CVD) Magnetic Bead Panel I immunoassay kits (Merck Millipore, USA). The cardiac biomarkers were treated as continuous variables29,33. Extreme values (exceeding three standard deviations from the mean) are adjusted by winsorizing and log-transformed to reduce skewness.
Social network survey
A complete sociocentric (global) network was constructed using the Korean version of the Social Network Survey name generator, which is identical to the NSHAP instrument used in the United States34. The question was read as follows:
From time to time, most individuals discuss things that are important to them with others. For example, these may include good or bad things that happen to you, problems you are having, or important concerns you may have. Looking back at the last 12 months, who are the individuals with whom you most often discussed things that were important to you?
In KSHAP, the social network includes the respondent’s discussion network (up to five individuals), plus their spouse if applicable. Therefore, network size ranges from 0 to 6 if including the spouse, or 0 to 5 otherwise. Unlike NSHAP, KSHAP listed spouses on the network roster first, followed by up to five additional members35. For each discussion partner, detailed information was collected including name, gender, age, address (rhee level), relationship type and duration, cohabitation status, education level, frequency of contact, and emotional closeness.
Constructing sociocentric network
To construct the sociocentric network, KSHAP used information from respondents’ egocentric network rosters—that is, the lists of people each respondent named as part of their social network. When the same individual was named by multiple respondents, we identified them as the same person if they matched on the following criteria: (1) at least two of the three Korean characters in their name, (2) gender, (3) age (within ± 5 years), and (4) residence in the same rhee (a small administrative unit). Using this approach, we assembled complete sociocentric networks for each wave of data collection (Waves 1, 4, and 5). Additional details on the matching procedure can be found in Youm et al. (2014) and Baek et al. (2023)31,35. Figure 1 presents the sociocentric network of the township. Node color represents BNP levels, with darker nodes indicating lower values. Node size reflects the number of college-educated individuals in each person’s network. The smallest black nodes represent discussion partners who lived in Township K but did not participate in the survey.

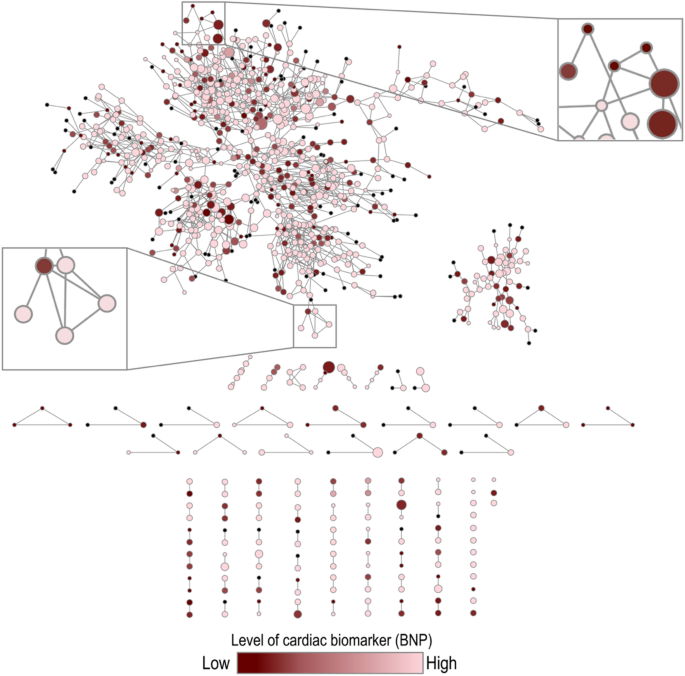
The socio-centric (complete) social network of Township K at the baseline n = 1,009). The color of the nodes represents the magnitude of each participant’s educational attainment of social network. The size of nodes represents the amount of BNP (smaller size → lower levels). The smallest black nodes represent discussion confidants living in Township K but did not participate in the survey.
Educational attainement of social networks
We measured the educational attainment of social networks by counting the number of individuals with a college degree or higher among respondents’ direct and indirect social ties.
Direct ties were defined as individuals named by respondents in response to name-generator questions during structured interviews. For each named alter, respondents reported detailed characteristics, including gender, age, relationship type, cohabitation status, and level of education. Education responses included: no education, informal education (soedang or hanhak), elementary school, middle school, high school, professional college, bachelor’s degree, and graduate degree. Direct ties were coded as college-educated if they had completed a bachelor’s degree or higher.
Indirect ties (friends of friends or second-degree ties) were identified using sociocentric (global) network data, which allowed us to observe the connections between alters. These individuals were not named by respondents directly but were connected to their named alters within the same village. We constructed measures of college-educated indirect ties using this sociocentric network data.
Variability is shown in Table S5: 7.5% of observations had one or more directly connected college-educated friends, and 12.8% had one or more college-educated friends of friends. Due to this distribution, we used a binary measure for direct ties and a categorical measure for second-degree ties in our analyses.
To avoid conflating the absence of social ties with the absence of college-educated ties, we excluded respondents who reported no ties. Sensitivity analyses that included these individuals yielded substantively similar results (Table S4).
Given prior evidence that geographically proximate and emotionally close ties are especially influential for health, we restricted our primary analyses to village-based networks—i.e., ties who resided in the same Township. Analyses of educational attainment among ties residing outside the Township did not show significant associations with cardiac biomarkers (Table S7).
We also examined the distinct associations of the educational attainment of friends of distance up to 4 and examine if they show a statistically significant relationship with cardiac biomarkers in our prospective data (Table S3).
Respondent’s educational attainment
Respondents reported their educational attainment during each wave of the survey. Response options included: no formal education, informal education (soedang or hanhak), elementary school, middle school, high school, professional college, bachelor’s degree, and graduate degree. Because education levels are unlikely to change in late adulthood, we used baseline reports to minimize recall error and inconsistency across waves. Respondent education was coded as a binary variable: 1 if they completed high school or higher, and 0 otherwise. We did not use college education as the threshold because only 3.1% had completed college.
Covariates
We controlled for potential the sociodemographic and health-related variables confounders. Sociodemographic covariates included annual household income and marital status (coded as 1 for living with a spouse, 0 otherwise). Income was coded as 1 for household earning approximately $10,000 or more per year, and 0 otherwise.
Health variables included comorbidity, cognitive functioning, physical health, smoking (1 for ever smoked, 0 otherwise), and hypertension diagnosis (1 for ever diagnosed, 0 otherwise). Comorbidity was defined as the number of diagnoses out of the following illnesses for each participant: diabetes, cancer, angina, cataracts, and osteoporosis. Cognitive function was assessed using the Korean version of the Mini-Mental State Examination for Dementia Screening (K-MMSE)47, with scores ranging from 0 to 30—higher values reflecting a better cognitive health status. Physical health statuses are assessed using the six-item physical component summary (PCS) from the SF-12 using standard methods.
We excluded participants who had been diagnosed with stroke, acute myocardial infarction (AMI), coronary heart disease (CHD), or angina over the study years to reduce potential reverse causation. We also excluded participants those with no social ties (n = 6). Sensitivity analyses including these cases yielded similar results (Table S4).
Statistical analysis
We used person-year fixed-effects regression models to examine within-individual changes in cardiac biomarkers as a function of educational attainment of social network and other covariates. This approach allows us to account for unobserved heterogeneity – difference in individual characteristics that are stable over time but not observed in our data (e.g. genetics, personalities, early-life conditions). This way, we control for these time-invariant confounders by reducing potential endogeneity and omitted variable bias36.
The Hausman test is conducted for all models to assess whether random-effects models are more acceptable. This test evaluates whether an explanatory variable is correlated with the error term, which signals the presense of endogeneity and violates assumptions of random-effects model37. In each case, the test indicates that unobserved heterogeneity is not randomly distributed, and therefore, the use of fixed-effect model is recommended.
We also perform several sensitivity analyses to check the robustness of our findings, which are available in supplemental material and briefly summarized in the results section. All analyses were conducted using Stata 18.0 (StataCorp LP, College Station, TX, USA).
link